Theories and Frames of Reference
Model
The Canadian Model of Occupational Performance and Engagement (CMOP-E) (Polotajko, Townsend, Craik, 2007) is generally an appropriate model to use when engaging individuals with cardiovascular disease in therapeutic interventions. This model reflects the various components of the person and their occupations, within an environment, in such a way that interventions can be client-centered and meaningful to each individual. Since cardiovascular disease is an umbrella term that includes a variety of conditions, the CMOP-E (Polotajko, Townsend, Craik, 2007) helps to investigate all factors impacting a person and their cardiovascular issues.
The following is a brief summary of possible interacting factors that an OT may consider when using the CMOP-E (Polotajko, Townsend, Craik, 2007) within a cardiovascular population. A visual representation of the model is also displayed.
Person:
Physical: Physical fitness level, hereditary factors, tobacco and alcohol consumption.
Affect: Emotional stress in relationships, combined with stressors at home and work, can take a toll on one's heart health.
Cognitive: After a heart attack or surgery, an individual may have cognitive impairment due to a temporary loss of oxygen to the brain.
Spiritual: Meditation and calming strategies are common stress relievers for people to try to work into their busy lives.
Occupation:
Self-care: Eating habits, lifestyle and routines, meal preparation, dental hygeine
Productivity: Job demands/ stressors
Leisure: Participating in enjoyable activities, taking time to relax and be active
Environment:
Physical: The design of the physical environment can enable or hinder individuals from engaging in physical fitness, for example, if an individual's work is within walking or biking distance, they may choose to do so, whereas in some locations this is not possible due to distance or weather.
Cultural: Cultural norms, such as exercise, desired body shape, and what is considered a healthy lifestyle vary immensely.
Institutional: Access to healthcare, and the quality and services provided varies across Canada, and even within cities.
Social: Social norms, such as drinking and smoking, lead to individuals consuming more and engaging in more unhealthy lifestyles.
The Canadian Model of Occupational Performance and Engagement (CMOP-E) (Polotajko, Townsend, Craik, 2007) is generally an appropriate model to use when engaging individuals with cardiovascular disease in therapeutic interventions. This model reflects the various components of the person and their occupations, within an environment, in such a way that interventions can be client-centered and meaningful to each individual. Since cardiovascular disease is an umbrella term that includes a variety of conditions, the CMOP-E (Polotajko, Townsend, Craik, 2007) helps to investigate all factors impacting a person and their cardiovascular issues.
The following is a brief summary of possible interacting factors that an OT may consider when using the CMOP-E (Polotajko, Townsend, Craik, 2007) within a cardiovascular population. A visual representation of the model is also displayed.
Person:
Physical: Physical fitness level, hereditary factors, tobacco and alcohol consumption.
Affect: Emotional stress in relationships, combined with stressors at home and work, can take a toll on one's heart health.
Cognitive: After a heart attack or surgery, an individual may have cognitive impairment due to a temporary loss of oxygen to the brain.
Spiritual: Meditation and calming strategies are common stress relievers for people to try to work into their busy lives.
Occupation:
Self-care: Eating habits, lifestyle and routines, meal preparation, dental hygeine
Productivity: Job demands/ stressors
Leisure: Participating in enjoyable activities, taking time to relax and be active
Environment:
Physical: The design of the physical environment can enable or hinder individuals from engaging in physical fitness, for example, if an individual's work is within walking or biking distance, they may choose to do so, whereas in some locations this is not possible due to distance or weather.
Cultural: Cultural norms, such as exercise, desired body shape, and what is considered a healthy lifestyle vary immensely.
Institutional: Access to healthcare, and the quality and services provided varies across Canada, and even within cities.
Social: Social norms, such as drinking and smoking, lead to individuals consuming more and engaging in more unhealthy lifestyles.
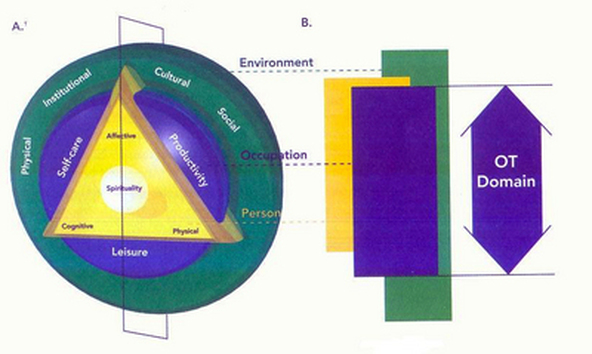
Canadian Model of Occupational Performance and Engagement, (Polotajko, Townsend, Craik, 2007)
Frames of Reference
Biomechanical
- Provide an upper extremity program to improve strength, range of motion, and endurance to help complete activities more independently while in the hospital and upon discharge.
- Provision of seating and positioning equipment
Rehabilitative (compensatory)
- Provide her with an ongoing rehabilitation program. Despite being in an acute care setting, clinical judgement can prove it is appropriate to offer rehabilitation right away to improve independence and function, and prepare rehabilitation program/ expedite discharge
A client-centred frame of reference should be used throughout the entirety of any intervention, focusing on individual goals and needs as much as possible to direct the treatment plan.
References
Polotajko, H.J., Townsend, E.A., Craik, J. (2007). Canadian Model of Occupational Performance and Engagement (CMOP-E). Enabling Occupation II, page 23.
Polotajko, H.J., Townsend, E.A., Craik, J. (2007). Canadian Model of Occupational Performance and Engagement (CMOP-E). Enabling Occupation II, page 23.
